
 English
English العربية
العربية Русский
Русский Français
Français Español
Español বাংলা
বাংলা Kiswahili
Kiswahili Deutsch
Deutsch 中文
中文 日本語
日本語 हिंदी
हिंदी

Macular Hole: What Patients Actually Need to Know
If your doctor has just told you that you have a macular hole, there’s a fair chance you’ve spent the last few hours trying to figure out what that actually means. And whether it’s as serious as it sounds.
Short answer: it’s not a hole in your eye. It’s a small break in a specific part of the retina. But it does need attention. The good news is that for most people who get it treated reasonably early, the outcome is genuinely good.
This guide covers the full picture , what causes it, what the symptoms are, how surgery works, and what recovery actually involves. Written for patients, not for a medical exam.
What Is a Macular Hole?
The macula is the small central zone of the retina at the back of your eye. It handles sharp, detailed vision , the kind you use for reading, recognising faces, and seeing fine detail. When a full-thickness break develops in this zone, that’s a macular hole.
It’s tiny. But because it sits right at the centre of the visual field, even a small hole causes noticeable problems.
Most develop with age , usually in people over 60. The vitreous gel inside the eye shrinks as we get older and gradually pulls away from the retina. Sometimes it pulls too hard on the macula. That traction is what creates the hole. Trauma can cause them too, but that’s far less common.
For patients travelling from the UK or US, this is one of the conditions where timing genuinely matters. Smaller, earlier-stage holes respond better to surgery and give better visual outcomes.

Symptoms: What Does It Feel Like?
The symptoms come on gradually, which is partly why people miss them at first. The things to watch for:
- Blurred or distorted central vision , straight lines look bent or wavy
- A grey or dark spot sitting in the middle of what you’re looking at
- Difficulty reading even with the right glasses
- Objects appearing smaller in the affected eye than the other
Crucially, peripheral (side) vision stays fine. The blur is specifically central. That’s one of the clearest signals that something is wrong with the macula rather than elsewhere.
Don’t wait to see if it settles. These symptoms don’t go away on their own. And the longer a hole is left, the harder it is to fix.
How Is It Diagnosed?
Diagnosis is usually quick once the right tests are done. The process looks like this:
- Pupil-dilating drops are used to open up the eye for examination
- The doctor examines the back of the eye directly
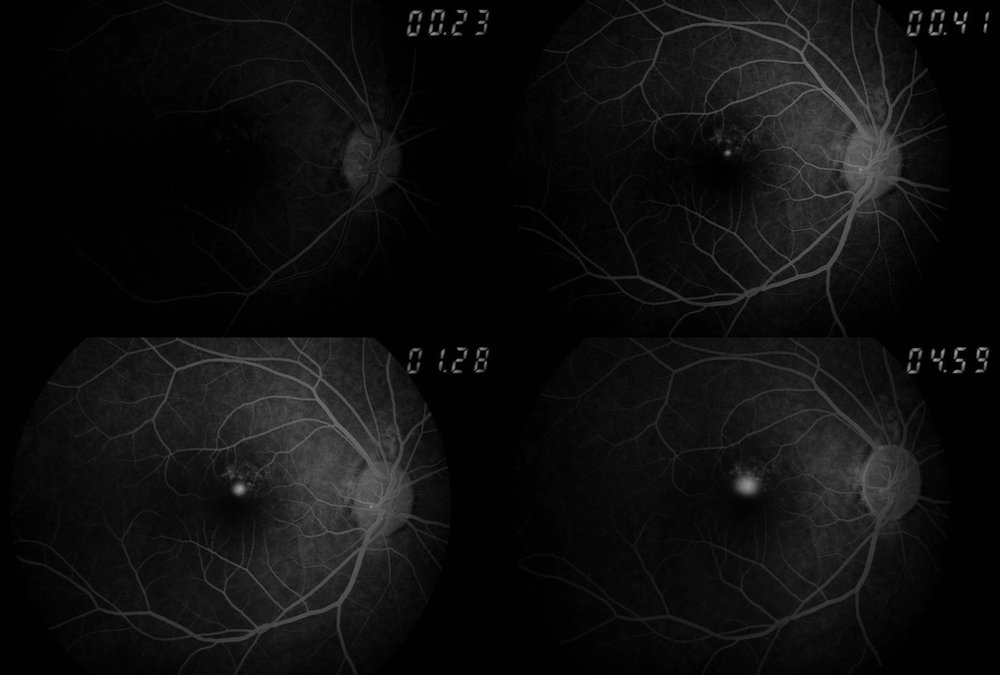
- An OCT scan is taken , this is the most important step
OCT (Optical Coherence Tomography) gives a detailed cross-sectional image of the retina. It shows exactly how large the hole is, how deep it goes, and what stage it’s at. This directly determines what treatment is needed.
There are four stages of macular holes. Stage 1 and 2 are smaller, more amenable to surgery, and more likely to give good visual recovery. Stage 3 and 4 are larger and longer-standing , they close less reliably and carry higher risk of partial recovery.
Catching it at stage 1 or 2 makes a real difference. That’s the whole reason not to delay.
Treatment: When Is Surgery Actually Needed?
Not every macular hole needs surgery right away. Some early or partial-thickness holes close on their own , your surgeon may recommend watching with repeat OCT scans for a period before deciding.
But for most full-thickness holes, surgery is the only thing that works. Drops, injections, or glasses don’t close a hole in the macula.
The surgery is called vitrectomy. Here’s what it involves:
- The vitreous gel is removed from inside the eye , see how vitrectomy surgeryis performed at Claritas
- The internal limiting membrane (a thin layer on the retinal surface) is carefully peeled , this is the most technically demanding part of the procedure
- A gas bubble is injected into the eye to press gently against the hole and help it seal
- The eye naturally refills with fluid over the following weeks as the bubble absorbs
Surgery takes roughly 30 to 60 minutes under local anaesthesia. Most patients go home the same day.
Results depend on three things: how long the hole has been present, how large it is, and the patient’s age. Long-standing large holes don’t always close completely. That’s the main reason timing matters.
Recovery After Surgery: The Part Nobody Loves
Face-down positioning. This is the bit people dread most, and it’s worth being honest about it: it’s uncomfortable. You’ll need to keep your face pointing downward for one to seven days, depending on the hole’s size.
But it’s not optional. The gas bubble needs gravity to sit against the correct part of the retina. Skipping or reducing the positioning reduces the chance of the hole closing properly.
What the weeks after surgery typically look like:
- Vision is blurry initially , that’s the gas bubble, not a complication
- The bubble gradually absorbs over two to eight weeks
- Vision slowly improves as the retina heals
- Most patients notice the biggest gains over the first three to six months
- Some continue improving up to a year post-surgery
Two absolute restrictions after surgery:
Flying. Do not fly while the gas bubble is in your eye. Cabin pressure causes the bubble to expand rapidly and can cause severe, irreversible damage. Your surgeon will confirm when flying is safe. For patients travelling from the UK or US, this planning is essential , factor in several weeks before your return flight.
Driving. You can’t drive until central vision meets the required standard. Your surgeon will check this at follow-up.
Risks: What Can Go Wrong?
Vitrectomy for macular holes has a high anatomical success rate. Most holes close. But closed doesn’t always mean perfect vision , some patients regain near-normal sight, others see partial improvement, and a small number see little change despite successful closure.
The risks worth knowing about:
- Cataract development , very common after vitrectomy, often within one to two years; it’s treatable
- Retinal detachment , rare, but needs prompt treatment if it happens; retinal detachment surgeryis available at Claritas
- Infection inside the eye (endophthalmitis) , rare but serious; caught early it’s manageable
- Raised intraocular pressure , usually temporary and treated with drops
Regular follow-up appointments aren’t just a box-ticking exercise. They catch these things early, when they’re fixable.
Practical Things Worth Knowing
A few points that come up a lot but don’t always get addressed:
- Tell your employer early if central vision is affected , screen adjustments, magnification software, or a change of tasks may help in the interim
- The other eye: people who develop a macular hole in one eye have a small but real risk in the other. Your surgeon will monitor both
- Diet doesn’t close an existing hole. But leafy greens, antioxidant-rich foods, and managing blood pressure and diabetes all support long-term retinal health
For patients considering treatment in India, Claritas provides support for the full journey , consultation, procedure, post-surgical care, and follow-up planning.
FAQs
What exactly is a macular hole?
A small full-thickness break in the macula, the central part of the retina that handles detailed vision.
What causes a macular hole?
Usually age-related shrinkage of the vitreous gel pulling on the retina; occasionally trauma.
What are the early signs?
Blurred central vision, distortion where straight lines look wavy, or a dark spot in the centre of sight.
Can it close without surgery?
Some early or partial-thickness holes do close on their own; full-thickness holes almost always need surgery.
How is it diagnosed?
An OCT scan after pupil dilation gives a precise image of the hole’s size, stage, and depth.
What surgery treats a macular hole?
Vitrectomy , removal of the vitreous gel, peeling of the internal limiting membrane, and a gas bubble to seal the hole.
How long is the face-down recovery?
One to seven days depending on the hole’s size; the gas bubble needs gravity to work.
Can I fly after the surgery?
No. The gas bubble expands at altitude and can cause severe, irreversible damage. Wait until your surgeon clears you.
What's the success rate?
Anatomical closure is achieved in most cases; vision improvement varies but the majority of patients do see gains.
How long does vision keep improving?
Improvement is gradual; most patients see the biggest change within three to six months, sometimes continuing up to a year.